

Introduction:
Pulmonary embolism (PE) is rare in childhood but a potentially fatal condition in the venous thromboembolism spectrum. However, the incidence of PE in children has been steadily increasing, which can be multifactorial. Adults data suggested that the finding of asymptomatic proximal DVT on routine ultrasonography is associated with increased mortality. Data on pulmonary embolism in children are scarce.
Objective:
To evaluate the relationship between asymptomatic proximal deep vein thrombosis detected in children presented with Pulmonary embolism.
Methods:
We conducted a retrospective chart review of all consecutive ICD 9 codes of Pulmonary Embolism (PE) in children over 10 years (January 1, 2000, to December 31, 2010) in Skåne university hospital in Sweden, using an electronic diagnosis hospital database. Eligible subjects were children aged 1-18 years presenting with PE diagnosed with imaging, and having undergone complete lower extremities radiological screening workup for DVT and lacking symptoms of acute lower extremity DVT. Data regarding subject demographics and medical history, risk stratification, low risk, massive or submissive PE, location of the proximal DVT, imaging method, presence of congenital vascular anomaly, time from symptom onset to diagnosis of the pulmonary embolism. Coagulation studies at primary investigation including at least plasma concentrations of protein C, protein S, antithrombin, resistance to activated protein C, and the genotypes FVG1691A and FIIG20210A. Also, plasma values for coagulation factors, VIII, cardiolipin antibodies, management, duration of anticoagulant, and the outcome were analyzed.
Results:
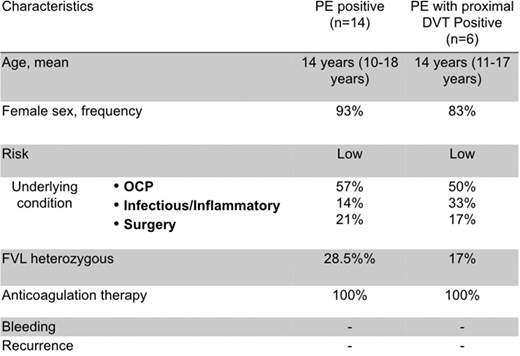
A total of 20 children enrolled. Age range 10-18 years (mean 15.8), 18 (90%) were female. Time from symptom onset to diagnosis of the PE: mean 4.8 days (range 1-28). All were low risk, and 6 (30%) associated with asymptomatic proximal DVT. The most common acquired risk factor was OCP/hormonal therapy was in 11 (55%). Minor thrombophilia in 5 (25%) of the cohort. All received anticoagulation therapy for 6 months, non-received pharmacologic thrombolysis. No bleeding, recurrence, nor thrombosis related mortality in 4 years follow uptime.
Conclusion:
PE is rare in children, and it is associated with asymptomatic proximal DVT is not uncommon. Our finding demonstrated the prevalence of PE associated with asymptomatic proximal DVT is 30%. This finding highlighted the importance of anticoagulant therapy for all patients with incidental proximal DVT.
No relevant conflicts of interest to declare.

